To be fair, I will copy Bryan's post from the HST FAQ on the subject of deconditioning.
<div></div><div id="QUOTEHEAD">QUOTE</div><div id="QUOTE">Though I wish I had more time to fully address your questions here, they will be more fully addressed in one of the HST books. In the mean time, we will try to use the most representative research of SD followed by retraining as we can find (with time constraints). The following study by Hortobágyi and colleagues (Hortobágyi, 2000) is one of the best I have found to date, with special reference to the adaptive changes to both deconditioning and retraining. Here is the full reference:
Hortobagyi T, Dempsey L, Fraser D, Zheng D, Hamilton G, Lambert J, Dohm L. Changes in muscle strength, muscle fibre size and myofibrillar gene expression after immobilization and retraining in humans. The Journal of Physiology 2000 April 1;524 Pt 1:293-304.
For those of you familiar with Medline the full text version is FREE.
But here are some important points brought to light by this and similar studies.
Deconditioning (including complete immobilization or even zero gravity)
1) In vivo studies suggest that a fall in the rate of protein synthesis rather than an increase in protein degradation is the predominant mechanism of atrophy at least during the first few weeks of immobilization in rats (Booth, F. W. & Seider, M. J. (1979). Early changes in skeletal muscle protein synthesis after limb immobilization of rats. Journal of Applied Physiology 47, 974-977) as well as in humans (Gibson, J. N. A., Halliday, D., Morrison, W. L., Stoward, P. J., Hornsby, G. A., Watt, P. W., Murdoch, G. & Rennie, M. J. (1987). Decrease in human quadriceps muscle protein turnover consequent upon leg immobilization. Clinical Science 72, 503-509)
2) In his pioneering work D. F. Goldspink (Goldspink, D. F. (1977). The influence of immobilization and stretch on protein turnover of rat skeletal muscle. The Journal of Physiology 264, 267-282) demonstrated that when the extensor digitorum longus of young rats was chronically stretched while immobilized, the muscle actually underwent hypertrophy. Although this chronic stretch may not be qualitatively equivalent to dynamic muscle lengthening, there is now cumulative evidence to suggest that strength gains (Dudley et al. 1991), muscle hypertrophy (Hather et al. 1991) and myosin heavy-chain (MyoHC) gene expression are specific to the type of mechanical loading (Booth & Thomason, 1991), with greater adaptations occurring if the mechanical stimulus contains muscle lengthening or eccentric contractions compared with concentric contractions.
3) Even though strength loss correlated with muscle fibre atrophy (r = 0·75), the magnitude of strength loss (47 %) was almost 4-fold greater than the magnitude of fibre atrophy (11 %) [with 3 weeks of immobilization]
4) Greater type II than type I muscle fibre atrophy occurred after elbow immobilization in the triceps brachii (30 vs. 25 %, MacDougall et al. 1980), in the vastus lateralis after an 11 day space flight (36 vs. 16 %, Edgerton et al. 1995), lower leg suspension (12 vs. 6 %, Berg et al. 1993) and knee immobilization (19 vs. 15 %, Veldhuizen et al. 1993). In contrast, others reported that atrophy was greater in type I than type II fibres (46 vs. 37 %, Sargeant et al. 1977; 26 vs. 1 %, Häggmark et al. 1981). In the present work type I and type II fibres atrophied to about the same extent, 13 and 10 %.
Retraining
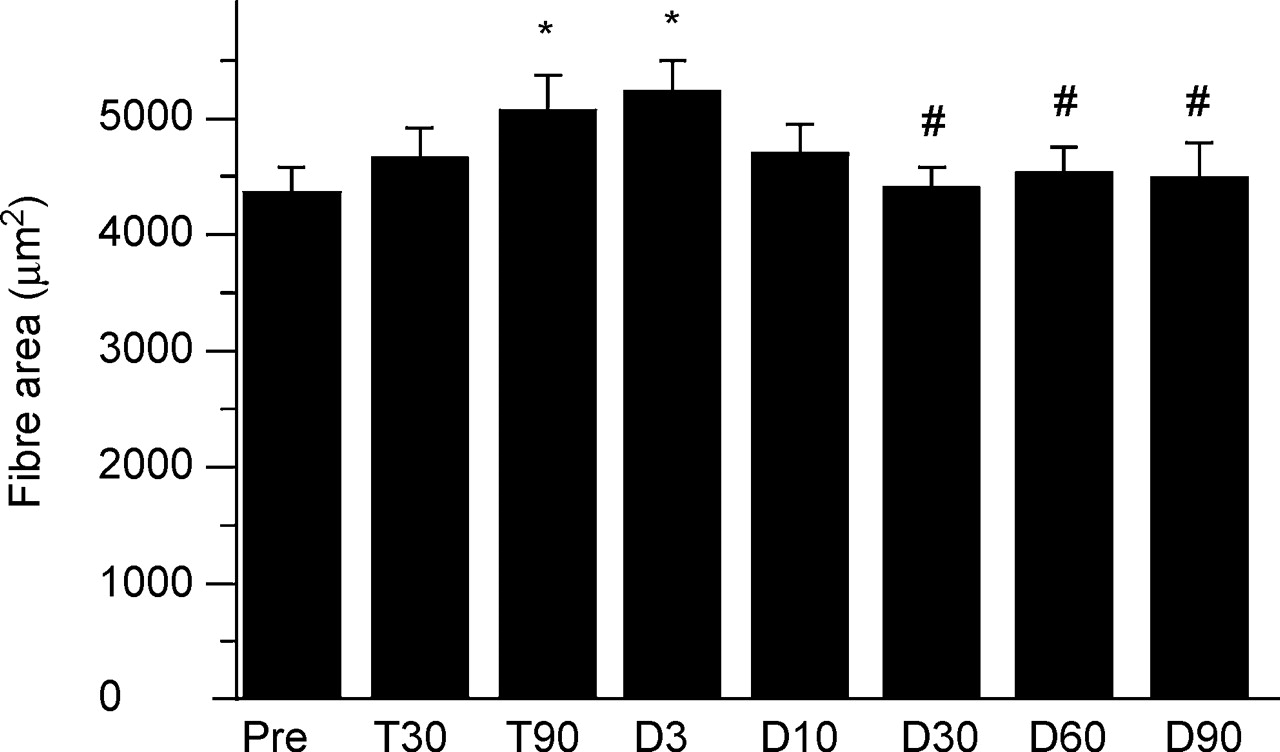
1) In the current work, resumption of spontaneous activity (i.e. just being up and around) for 2 weeks after the cast was removed resulted in about 90 % recovery of muscle strength and 95 % recovery of muscle fibre size. [That’s an 10% increase in muscle size in only two weeks WITH NO TRAINING!]
2) 3 weeks of immobilization significantly and uniformly reduced type I, IIa and IIx muscle fibre areas by 13, 10 and 10 %, respectively…Hypertrophy of type I, IIa and IIx fibres relative to baseline was 10, 16 and 16 % after eccentric and 11, 9 and 10 % after mixed training (all P < 0·05) and these gains were significantly (P < 0·05) greater than the hypertrophy after concentric training (4, 5 and 5 %). In addition, the type IIa and IIx fibres were significantly larger after eccentric than after mixed training
3) We observed a significantly faster rate of strength recovery when the exercise program contained eccentric contractions. Muscle strength recovery after 4 weeks was complete when subjects exercised with concentric contractions, whereas recovery to initial levels occurred about 2 weeks faster when pure eccentric contractions were used or added to concentric contractions…Not only was the rate of strength recovery faster with pure eccentric or mixed eccentric and concentric contractions but the strength gains and muscle fibre hypertrophy were also substantially greater compared with pure concentric contractions, confirming most (Komi & Buskirk, 1972; Dudley et al. 1991; Hather et al. 1991; Hortobágyi et al. 1996a, b) but not all (Jones & Rutherford, 1987; Smith & Rutherford, 1995) prior reports. [We are not so interested in strength, but this info is demonstrative of the importance of eccentric training.]
Now this doesn’t speak much towards RBE, but it does demonstrate how muscle tissue responds differently after SD than it does during training. It’s a sliding scale of sensitivity and hypertrophy. When muscle is at its highest sensitivity, it grows most rapidly, and likewise, it grows more resistant to further growth at the same rate. I have other studies on RBE that I may be able to post later.
1. McHugh MP. Recent advances in the understanding of the repeated bout effect: the protective effect against muscle damage from a single bout of eccentric exercise. Scand J Med Sci Sports. 2003 Apr;13(2):88-97.
2: Thompson HS, Clarkson PM, Scordilis SP. The repeated bout effect and heat shock proteins: intramuscular HSP27 and HSP70 expression following two bouts of eccentric exercise in humans. Acta Physiol Scand. 2002 Jan;174(1):47-56.
3: Proske U, Morgan DL. Muscle damage from eccentric exercise: mechanism, mechanical signs, adaptation and clinical applications. J Physiol. 2001 Dec 1;537(Pt 2):333-45.
4: Stupka N, Tarnopolsky MA, Yardley NJ, Phillips SM. Cellular adaptation to repeated eccentric exercise-induced muscle damage. J Appl Physiol. 2001 Oct;91(4):1669-78.
5: McHugh MP, Connolly DA, Eston RG, Gleim GW. Exercise-induced muscle damage and potential mechanisms for the repeated bout effect. Sports Med. 1999 Mar;27(3):157-70.
6: Brown SJ, Child RB, Day SH, Donnelly AE. Exercise-induced skeletal muscle damage and adaptation following repeated bouts of eccentric muscle contractions. J Sports Sci. 1997 Apr;15(2):215-22.
7: Brown SJ, Child RB, Day SH, Donnelly AE. Indices of skeletal muscle damage and connective tissue breakdown following eccentric muscle contractions. Eur J Appl Physiol Occup Physiol. 1997;75(4):369-74.
8: Ebbeling CB, Clarkson PM. Exercise-induced muscle damage and adaptation. Sports Med. 1989 Apr;7(4):207-34.
- Bryan Haycock</div>