 |
|
|
Creatine: The Ergogenic / Anabolic Supplement
Mesomorphosis Magazine
September 1998 (Volume 1, Number
4)
by Richard B. Kreider, PhD, FACSM
rkreider@memphis.edu
Please send us your feedback
on this article.
Overview
Scientific studies indicate that creatine supplementation is an
effective and safe nutritional strategy to promote gains in strength and
muscle mass during resistance-training. Moreover, that creatine
supplementation may be an effective alternative to other less effective
and/or potentially dangerous nutritional and pharmacological strategies
that athletes have used in an attempt to increase strength and muscle
mass during training. Consequently, creatine has become one of the most
popular nutritional supplements for resistance-trained athletes and body
builders. Yet despite the scientific evidence, there has been a
significant amount of controversy about creatine reported in the popular
media. This article will examine what we do and don’t know about
creatine and whether concerns about side effects reported in the popular
media have any merit.
What is
Creatine?
Creatine is a naturally occurring amino acid which is derived from
the amino acids glycine, arginine, and methionine. The body stores
creatine in both free and phosphorylated forms. The average sized person
(70 kg) stores about 120 g of creatine.7,17,49,59,60,77,121
Most of the creatine is stored in skeletal muscle (95%) primarily as
phosphocreatine (66%) while the remaining amount of creatine is found in
the heart, brain, and testes.7,17,49,60,121 The normal daily
requirement for creatine is about 1.6% of the total creatine pool (about
2 to 3 g/d for a 70 to 100 kg individual). About half of the daily needs
of creatine are typically obtained from the diet primarily from meat,
fish, and animal products. For example, there is about 1.4 to 2.3 g of
creatine per pound of meat (beef, pork) or fish (tuna, salmon, cod).
Herring contains about 3 to 4.5 g of creatine per pound. Creatine can
also be obtained by supplementing the diet with pharmacological grade
synthetic creatine. The most popular and economical form of synthetic
creatine is creatine monohydrate (creatine plus one molecule of water).
When dietary availability of creatine is insufficient to meet daily
needs, the remaining creatine is synthesized from the amino acids
glycine, arginine and methionine primarily in the liver, kidney and
pancreas (refer to Figure 1).7,17,49 This first involves the
reversible transfer of an amidine group from arginine to glycine to form
guanidinoacetic acid. This is then followed by an irreversibly transfer
of a methyl group from S-adenosylmethionine to guanidinoacetic acid
forming creatine. When dietary availability of creatine is low,
endogenous synthesis of creatine is increased to maintain normal levels.
On the other hand, when dietary availability of creatine is increased,
endogenous creatine synthesis is temporarily suppressed. 7,17,49
See Figure 1.
How
Does Creatine Work?
The energy for all out maximal effort exercise lasting up to 6 to 8
seconds is primarily derived from limited stores of adenosine
triphosphate (ATP) in the muscle. In this regard, the phosphate from ATP
is cleaved off liberating energy for muscle contraction. During
explosive exercise, the phosphate from phosphocreatine (PCr) stored in
the muscle is also cleaved off to provide energy for resynthesis of ATP.
This allows the ATP pool to be turned over several dozen times during an
all out maximal effort exercise bout lasting 6 to 8 seconds.
Additionally, the energy derived from the breakdown of PCr during
recovery helps restore the ATP depleted during maximal effort explosive
exercise.
Creatine supplementation has been suggested as a means to
"load" the muscle with creatine and PCr in a similar way that
endurance athletes "load" their muscle with carbohydrate.59,60,121
Loading the muscle with creatine and PCr would theoretically serve to
improve the ability to produce energy during high intensity exercise as
well as improve the speed of recovery. Theoretically, this would help an
athlete perform more work during a single bout of high intensity
exercise and recover faster between multiple sets of high intensity
exercise.
Well, so much for the theory. There are lots of supplements sold to
athletes that sound great in "theory". The bottom line for the
athlete is does it work? Is the supplement safe? And, is the supplement
worth the money? Unlike most supplements you find at your local health
food store, there has been a great deal of research investigating the
effects of creatine supplementation on muscle energy production and
exercise performance. If fact, with the exception of carbohydrate,
creatine has been the most extensively studied nutrient sold to
athletes.
Studies investigating the effects of dietary creatine supplementation
actually began in the early 1920s.17 Although initial studies
reported some ergogenic benefit, elite athletes didn’t begin using
creatine as a nutritional supplement until the 1960s (particularly in
the Eastern block countries of the former Soviet Union). In the mid- to
late 1980s, creatine became a popular nutritional supplement among elite
athletes in Europe and Great Britain. However, its widespread used among
the general athletic communities didn’t occur until the early to mid
1990's when synthetic creatine was marketed in the U.S. more affordably.59,60,121
As of this writing, there have been about 70 original research
articles published in peer-reviewed journals on creatine supplementation
with another 50 or so papers presented in the last few years at various
scientific meetings. These studies indicate that short-term creatine
"loading" (15 to 30 g/d or 0.3 g/kg/d for 5 to 7-d) increases
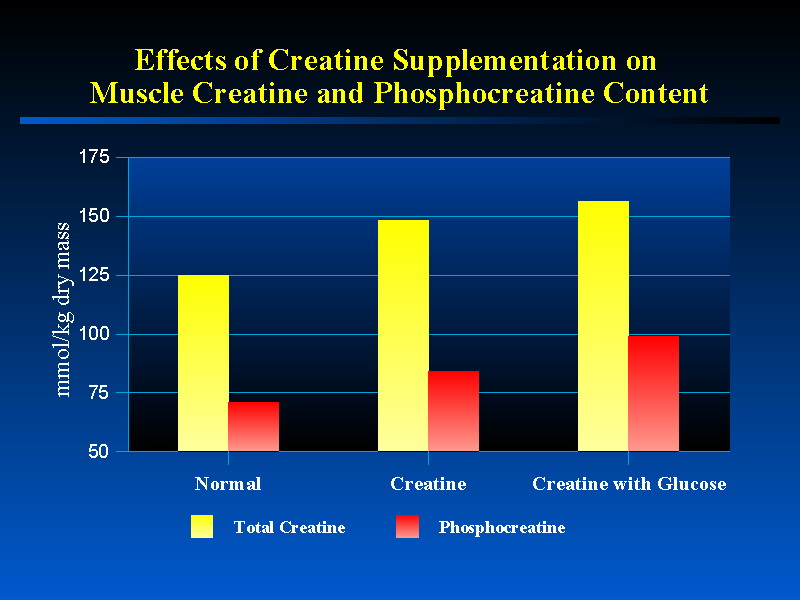
total creatine content (TCr) by 15 to 30% and PCr stores by 10 to 40%.8,11,15,16,32,38,39,40,42,43,47,50,69,70,72,79,
91,92,115 For example, Harris and coworkers 47 reported
that ingesting 20 to 30 g/d of creatine for 5-, 7- and 10-d or on
alternate days for 21-d increased TCr by 20% (127 to 149 mmol/kg dry
mass) and PCr by 36% (67 to 91 mmol/kg dry mass). Likewise, Balsom and
associates8 reported that creatine supplementation (20 g/d
for 6-d) increased muscle TCr by 18% (129 to 152 mmol/kg dry mass). An
alternative strategy of increasing muscle creatine content is to ingest
small amounts of creatine per day (3 g/d) for 28-d. This results in a
more gradual increase in TCr and PCr concentrations over time.50
Studies show that the greatest amount of creatine uptake occurs during
the first 3- to 5-d of ingesting loading doses.47,50 The
elevated levels of muscle TCr and PCr can be maintained thereafter by
ingesting 2 to 5 g/d.50,115 Following cessation of creatine
supplementation, TCr and PCr levels return toward baseline levels in 28-
to 35-d.32,72,115
Although all studies have reported increases in muscle TCr and PCr
levels following creatine loading (i.e., 20 g/d for 5-d), there is some
evidence that not all individuals respond as well to creatine loading as
others (i.e., observe less than a 20 mmol/kg dry mass increase in TCr
levels). Further, that "non-responders" experience less of an
improvement in exercise performance following creatine supplementation.43,47
In this regard, studies suggest that some subjects (20 to 30%) only
increase TCr and PCr levels by 5 to 15% in response to creatine loading
(20 g/d for 5-d) and that these subjects experience less of an
improvement in exercise capacity than subjects experiencing greater than
20% increase in TCr and PCr. This "non-responder" phenomenon
has been suggested to be due to possible differences in storage rates or
initial creatine content among people. However, more recent studies 39,40
indicate that if you ingest creatine (20 g/d) with large amounts of
glucose (380 g/d) during the first 5-d loading period, muscle creatine
content was increased by 10% more than when creatine was ingested alone
(143 to 158 mmol/kg dry mass). This allowed all subjects to experience
large increases in muscle creatine content and performance.
Additionally, these investigators found that when creatine was ingested
with glucose, glycogen content was increase by 18% more than when
glucose was ingested alone (418 to 489 mmol/kg dry mass). While this
change was not significantly different, gains in glycogen were
significantly correlated with gains in TCr suggesting that the increases
in glycogen observed were at least in part due to creatine. This is the
reason why it is recommended that athletes ingest creatine with glucose
or fruit juice. Figure 2 presents the average changes in TCr and PCr
reported in the literature in response to creatine supplementation with
and without glucose.
See Figure 2.
Since creatine supplementation can increase intramuscular PCr
concentrations, creatine supplementation would theoretically enhance the
availability of energy during explosive, high-intensity exercise bouts
and/or enhance the ability to recover from intense exercise. For this
reason, a number of studies have evaluated the effects of creatine
supplementation on ATP and PCr concentrations during and following
high-intensity exercise.8,15,16,32,42,43,72,115 These studies
indicate that creatine supplementation does not appear to alter
pre-exercise ATP concentrations.32,47 However, the elevated
PCr concentrations serve to maintain ATP concentrations to a greater
degree during maximal effort high intensity exercise.16 In
addition, creatine supplementation appears to enhance the rate of ATP
and PCr resynthesis following intense exercise.8,15,16,32,42,43,72,115
Since resistance-training involves performance of multiple sets of
moderate to high intensity exercise, creatine supplementation would
theoretically allow a weight lifter/body builder to increase work output
during multiple sets of resistance-exercise leading to greater gains in
strength and/or muscle mass.
Does Creatine
Enhance Exercise Performance?
Most studies (about 70 to 80%) which have investigated the ergogenic
value of short-term (5 to 7-d) and/or long-term (7 to 140-d) creatine
supplementation (20 to 25 g/d for 5 to 7-d and 2 to 25 g/d thereafter)
have reported that creatine supplementation significantly increases
strength/power, sprint performance, and/or work performed during
multiple sets of maximal effort muscle contractions. The improvement in
exercise capacity has been attributed to increased TCr and PCr content .8,15,16,32,39,40,42,43,47,50,69,72,79,91,92,114,115,116
particularly in type II muscle fiber,16,79 greater
resynthesis of PCr, 8,16,42,72,92,115 improved metabolic
efficiency, 5,8,16,12,44,80 and/or an enhanced quality of
training promoting greater training adaptations.1,12,33,37,45,56,57,62-65,73,84,91,104
The following analysis overviews some of the literature reporting
ergogenic benefits of creatine supplementation. Additionally, Table 1
summarizes results of studies evaluating the ergogenic value of creatine
supplementation. For a more detailed analysis of these and other
studies, see Tables 1 through 3 in a review recently published 59
in the Journal
of Exercise Physiology Online.
| Table 1. Summary of the types of exercise and/or exercise
conditions in which creatine supplementation has been reported to
provide ergogenic benefit. |
| One Repetition Maximum and/or Peak Power 10,12,24,28,29,38,44,54,56,57,65,74,76,82,89,94,115,116,117,119,120,124 |
| Vertical Jump 13,37,104 |
| Work Performed During Multiple Sets of Maximal Effort Muscle
Contractions 1,3,13,29,38,44,46,54,64,69,72,98,115,116,117 |
| Single Sprints/Maximal Effort Contractions Lasting 6 to 30-s 1,8,12,16,28,29,33,44,45,70,87,94,104,124 |
| Repetitive Sprints (recovery 0.5 to 5-min) 1,5,8,12,24,27,29,31,33,48,55,57,64,73,74,85,91,109,124 |
| High Intensity Exercise Lasting 1.5 to 10-min 26,27,30,48,97 |
| Increased Ventilatory Anaerobic Threshold 80 |
| Increase Maximal Exercise Capacity 52 |
Maximum Strength/Power
For a weight lifter/body builder, gains in strength/power are often
accompanied by muscle hypertrophy. Consequently, ingesting a nutritional
supplement which can promote strength gains during training may be
particularly beneficial. Studies indicate that creatine supplementation
during training can increase gains in one repetition maximum (1RM)
strength and/or power.10,12,24,28,29,38,44,54,56,57,65,74,76,89,94,115,116,117,120,124
For example, Earnest and associates 29 reported that 28-d
of creatine supplementation (20 g/d for 28-d) during resistance-training
promoted a significantly greater gain in 1RM bench press performance (8.2
kg) compared to subjects ingesting a placebo during training (-2.9 kg).
Likewise, Vandenburghe and colleagues 116 reported that
creatine supplementation (20 g/d for 4-d followed by 5 g/d for 66-d)
promoted a 20 to 25% greater gain in 1RM strength in untrained women
participating in a 70-d resistance-training program than subjects
receiving a placebo. Furthermore, the gains in strength observed were
maintained in subjects ingesting creatine during a 70-d detraining period.
These findings indicate that creatine supplementation during
resistance-training promotes significantly greater gains in strength.
While it is understandable that if creatine allows an athlete to train
harder that athletes may get stronger over time, studies also indicate
that short-term creatine supplementation may enhance peak power.12,24,38,44,54,57,124
For example, Dawson and coworkers 24 reported that creatine
supplementation (20 g/d for 5-d) significantly increased peak power during
the first set of 6 x 6-s sprints. Birch and colleagues 12
reported that creatine supplementation (20 g/d for 5-d) significantly
increased peak power output (8%) during three sets of 30 maximal effort
cycling sprints. Moreover, short-term creatine supplementation has been
reported to increase peak concentric and eccentric power 54 as
well as vertical jump performance.13,37,104 These findings are
interesting in that peak power generated during a single explosive
exercise (e.g. 1 RM) is not greatly dependent on the amount of ATP and PCr
in the muscle. To increase power, one has to generate more force in a
shorter period of time which usually occurs in response to muscle
hypertrophy and/or enhanced neural adaptations to training. Consequently,
since the availability of ATP and PCr are not limiting factors to an
explosive 1RM, one would not expect short-term creatine supplementation to
improve peak power. Yet, several studies indicate that short-term creatine
supplementation can increase peak power and/or 1RM strength. These
findings have led researchers to wonder if short-term creatine
supplementation may affect the peripheral nervous system.
Multiple Sets of Maximal Effort Muscle
Contractions
One of the potentially most beneficial effects of creatine
supplementation for the weight lifter/body builder is that creatine
supplementation has been reported to increase the amount of work performed
during a series of maximal effort muscle contractions. 1,3,13,29,38,44,46,54,64,69,72,98,115,116,117,122
For example, Bosco et al 13 found that creatine supplementation
(20 g/d for 5-d) significantly increased jump performance during two 15-s
jump tests separated by a 15-s rest recovery. Volek and colleagues 116
reported that creatine supplementation (25 g/d for 7-d) resulted in a
significant increase in the amount of work performed during five sets of
bench press and jump squats in comparison to a placebo group. Moreover,
Earnest and associates 29 found that creatine supplementation
(20 g/d for 28-d) significantly increased bench press total lifting volume
(43%) when performing a 70% of 1 RM bench press repetition test. Finally,
Kreider et al.64 reported creatine supplementation (15.75 g/d
for 28-d) promoted a 41% greater gain in combined bench press, squat, and
power clean lifting volume. These findings suggest that creatine
supplementation may enhance the ability to perform sets of multiple effort
muscle contractions thus serving to increase the quality of workouts.
Sprint/High-Intensity
Performance
Creatine supplementation has also been reported to improve single
effort 1,8,12,16,28,29,33,44,45,70,87,94,104,123 and/or
repetitive sprint performance 1,5,8,12,24,27,29,31,33,48,55,57,64,71,73,74,85,91,109,121,123
particularly in sprints lasting 6 to 30-s with 30-s to 5-min of rest
recovery between sprints. For example, Birch et al 12 reported
that creatine supplementation (20 g/d for 5-d) significantly increased
work performed during the first of 3 x 30-s cycle ergometer sprints with
4-min recovery between sprints. Grindstaff and coworkers 45
reported that creatine supplementation (21 g/d for 9-d) significantly
improved 3 x 100-m swim performance with 60-s rest recovery between
sprints. Moreover, Kreider and associates 64 reported that 28-d
of creatine supplementation (15.75 g/d) during off-season football
resistance/agility training resulted in significant improvements in
repetitive sprint performance during the first five of 12 x 6-s sprints
with 30-s rest recovery between sprints. Finally, Earnest and colleagues 29
reported that creatine supplementation (20 g/d for 28-d) increased work
performed during 3 x 30-s cycle ergometer sprints with 5-min rest recovery
between sprints. While not all studies indicate that creatine
supplementation improves single and/or repetitive sprint performance (see
discussion below), these studies suggest that creatine supplementation may
improve single and/or repetitive sprint performance.
Although exercise involving the ATP-PC energy system (i.e.,
high-intensity single and/or repetitive sprint performance lasting up to 8
seconds) would theoretically receive the most benefit from creatine
supplementation, some investigators have studied whether creatine
supplementation would affect high-intensity exercise performance lasting
60-s to 10-min in duration.14,26,27,30,32,48,97,108 The
rationale for this is that often the latter portions of high-intensity
exercise performance lasting 60-s to 10-min often involves all out sprint
performance. Consequently, if creatine loading enhances sprint
performance, it may provide some ergogenic benefit in longer events which
also require sprint performance at the end of the events. There are
several studies supporting this theory. In this regard, Harris and
coworkers 48 reported that sprint performance during a series
of 300- and 1,000-m runs were significantly improved with creatine
supplementation (30 g/d for 6-d). Earnest and colleagues26,27
and Smith et al. 97 found that creatine supplementation
significantly increased high intensity exercise performance lasting up to
600-s in duration. Moreover, Rossiter et al.91 reported that
creatine supplementation (0.25 g/kg/d for 5-d) significantly decreased
time to perform a 1,000-m rowing time trial by 2.3-s in an event lasting
about 210-s in comparison to a placebo group. Finally, Jacobs and
associates52 reported that creatine supplementation
significantly increased time to exhaustion by 8% (130 to 141-s) following
5-d of creatine supplementation (20 g/d) as well as following 7-d
cessation of supplementation by 7% (139-s). Although additional research
is necessary, these findings suggest that creatine supplementation may
provide some ergogenic benefit in events lasting up to 10-min. Collectively,
these findings suggest that if your involved in more than just weight
lifting/body building (as most resistance-trained athletes are), creatine
may improve your ability to sprint, recover from sprints, and perform
high-intensity exercise lasting up to 10-min in duration.
Endurance Performance
Although the ATP-PC energy system is not highly involved in submaximal
endurance exercise performance, several studies have evaluated the effects
of short-term creatine supplementation on submaximal endurance exercise
performance.6,31,36,79 These studies indicate that short-term
creatine supplementation does not appear to improve submaximal exercise
performance. In fact, Balsom and colleagues 6 reported that
6-km run performance may be negatively affected theoretically due to an
increase in body mass. Consequently, creatine supplementation is generally
not recommended for endurance athletes.
However, it should be noted that no long-term studies have been
conducted on the effects of creatine supplementation in endurance
athletes. It is my view that there may be some potential benefits of
creatine supplementation for endurance athletes that warrant additional
research. In this regard, creatine supplementation has been reported to
increase repetitive sprint performance, muscle mass, and enhance glycogen
uptake when creatine is ingested with large amounts of glucose.
Consequently, creatine supplementation may help an endurance athlete by
improving interval performance capacity during training, maintain muscle
mass during training, and/or serve as an effective way to load the muscle
with glycogen. Additionally, creatine supplementation has been shown to
help athletes tolerate training to a greater degree. Over time, this may
lead to improved endurance performance capacity and/or a reduction in the
incidence of overtraining.
Studies Reporting No
Ergogenic Benefit
Although most studies (about 70 to 80%) have reported statistically
significant improvement in exercise performance in response to short
and/or long-term creatine supplementation, some well-controlled studies
have reported no ergogenic benefit from creatine supplementation (see
table 2). The reason for the lack of ergogenic effect of creatine
supplementation observed in these studies is not clear. However, it is
possible that individual variability in response to creatine
supplementation previously discussed may account for the lack of ergogenic
benefit reported in these studies.43,47 It is also possible
that differences in experimental design may account for some of the
differences in results observed. In this regard, creatine supplementation
appears to be less ergogenic when supplementation regimens are less than
20 g/d for 5-d 9,53,92,81 or involve low-dose supplementation
regimens (2 to 3 g/d) without an initial higher dose loading period.44,52
In addition, studies which used relatively small sample sizes (e g., <
6 subjects per group) or employed crossover experimental designs with less
than a 5-wk washout period between trials typically have found no
ergogenic benefit.32,72,81,92 Creatine supplementation may also
be less ergogenic depending on the amount of work performed and rest
recovery observed between repetitive exercise trials. Several studies
report that creatine supplementation does not effect performance in
sprints lasting 6- to 60-s when prolonged recovery periods (5- to 25-min)
are observed between sprint trials.14,22,78,90 Finally,
short-term creatine supplementation does not appear to enhance
endurance exercise.31,36,79 Consequently, although most studies
indicate that creatine supplementation may improve performance, creatine
supplementation may not provide ergogenic value for everyone.
| Table 2. Summary of types of exercise and/or exercise
conditions in which creatine supplementation has been reported to
provide no ergogenic benefit. |
| One Repetition Maximum or Peak Force 4,46,98,106,119,122 |
| Vertical Jump 76 |
| Work Performed During Multiple Sets of Low Intensity or Maximal
Effort Muscle Contractions 35,69,82,89,110,106 |
| Single Sprints Lasting 6 to 30-s 13,24,37,53,81,85,92 |
| Repetitive Sprints (recovery 30- to 120-s 51 and 5- to 25-min) 9,14,21,22,78,90,94,96,111,114 |
| Exercise Lasting 60-220-s 14,32,108 |
| Submaximal Endurance Exercise 31,36,79,105 |
Does
Creatine Affect Muscle Mass?
So creatine may improve your ability to train harder and recover
faster from multiple sets during your workouts. Does it really increase
muscle mass? If so, are gains modest or impressive? Is creatine really
an nutritional alternative to other anabolic agents or just another
overly hyped supplement?
Most studies indicate that short-term creatine supplementation (20 to
25 g/d for 5 to 7-d) increases total body mass by approximately a 0.7 to
1.6 kg (see Table 3).5,6,8,40,43,72,75,78,89,109,115,116,123
In addition, a number of long-term (7 to 140-d) studies investigating
the effects of creatine or creatine containing supplements (20 to 25 g/d
for 5 to 7-d and 2 to 25 g/d thereafter) on body composition alterations
during training have reported significantly greater gains in total body
mass regimens 10,29,37,57,61,63,66,77,84,95,104,115 and
fat-free mass.10,29,56,57,61,63,65,66,74,75,84,104,115 The
gains in total body mass and fat-free mass (FFM) observed were typically
0.8 to 3 kg greater than matched-paired controls depending on the length
and amount of supplementation. For example, Kreider et al.64
reported that 28-d of creatine supplementation (15.75 g/d) resulted in a
1.1 kg greater gain in FFM in college football players undergoing
off-season resistance/agility training. In addition, Vandenburghe and
coworkers115 reported that untrained females ingesting
creatine (20 g/d for 4-d followed by 5 g/d for 66-d) during
resistance-training observed significantly greater gains in FFM (1.0 kg)
than subjects ingesting a placebo during training. Moreover, the gains
in FFM observed were maintained while ingesting creatine (5 g/d) during
a 10-week period of detraining as well as following 4-weeks cessation of
supplementation. Finally, preliminary data presented at the 1998
National Strength and Conditioning annual meeting from Dr. Bill Kraemer’s
laboratory at Penn State University indicated that creatine
supplementation (25 g/d for 7-d followed by 5 g/d for 77-d) promoted
significant increases in muscle mass which was accompanied by an
approximately 30% increase in type I and type II muscle fiber diameter.
Collectively, these findings provide convincing evidence that creatine
supplementation during training promotes muscle hypertrophy.
| Table 3. Effects of Creatine on Body Mass and Composition |
| Significant Increase in Total Body Mass Following Short-term
Supplementation Regimens 5,6,8,40,43,72,75,78,89,109,115,116,122 |
| No Significant Effect on Total Body Mass or Fat Free Mass
Following Short-term Supplementation Regimens 25,36,45,46,76,90,108,116 |
| Significant Increase in Total Body Mass Following Long-term
Supplementation Regimens 10,29,37,57,61,63,66,77,84,95,104,116 |
| Significant Increase in Fat Free Mass following Short- and/or
Long-term Creatine Supplementation 10,29,56,57,61,63,65,66,74,75,77,84,104,116,121,124 |
| No Significant Changes in Fat Free Mass following Short- and/or
Long-term Creatine Supplementation 122 |
Although the majority of studies report that creatine supplementation
increases body mass and/or lean body mass, the mechanism in which
creatine supplementation may affect gains in body mass and/or fat free
mass is not entirely clear. Nevertheless, there are three prevailing
theories. First, since gains in body mass (about 1 kg) can occur within
3 to 7-d, some suggest that the gains in body mass observed are simply
due to greater water retention. In support of this contention, initial
studies reported that urine output declined during the first three days
of creatine supplementation suggesting greater fluid retention.50
Additionally, recent papers suggests that intracellular fluid volume
increases during the first 3-d of creatine supplementation.56,123,124
Yet, other studies which have evaluated the effects of long-term
creatine supplementation on total body water have reported that the
increases in total body water are proportional to the gains in weight
(i.e., the percentage of total body water is not significantly changed).63,64,66,108
In this regard, since muscle is approximately 70% water, an increase of
3 kg of muscle should be accompanied by 2.1 kg increase in body water.
Consequently, although total body water may increases, it does not
increase the percentage of total body water. Further, although initial
gains in body mass can be explained to some degree by increases in total
body water, the magnitude of change in muscle mass which has been
reported in response to chronic creatine supplementation during training
(mean changes as great as 5.5 kg in 6-weeks) argues against this theory.
This is especially true when one considers that the gains in mass are
typically accompanied by greater gains in strength, power, and/or sprint
speed.
Second, creatine supplementation has been reported to affect protein
synthesis.7,11,51,112,124 This theory suggests that an
initial creatine stimulated gain in intracellular water may serve to
increase osmotic pressure which in turn stimulates protein synthesis.
There is some preliminary evidence to support this hypothesis.11,83,123
For example, Ziegunfuss et al.123 reported that nitrogen
status was increased in a subset of subjects following 3-d of creatine
supplementation suggesting that creatine increases protein synthesis
and/or may decrease net protein breakdown. Kreider et al.64
reported that the ration of urea nitrogen to creatinine (a general
marker of anabolic/catabolic status) was decreased in athletes ingesting
creatine (15.75 g/d for 28-d). Although additional research is
necessary, these findings suggest that creatine supplementation may
affect protein synthesis and/or reduce whole body catabolism during
training.
Finally, some suggest that since creatine may allow an athlete to
train harder, the enhanced training stimulus may promote greater muscle
hypertrophy over time. Although this theory makes a lot of sense and can
explain the increases in muscle mass reported in long-term studies, it
should be noted that significant increases in muscle mass have been
observed in as little as one week following creatine supplementation.
Consequently, it is my view that the gains in muscle mass observed are
most likely due to a combination of these theories.
Is Creatine
Safe?
Although there is strong evidence that creatine supplementation can
improve exercise performance and lead to greater gains in muscle mass,
concerns have been recently raised about potential side effects and/or
the long-term safety of taking creatine. I am sure you have seen the
headlines, read the newspapers, or heard reporters on television warn
you about the side effects of creatine. Things like creatine causes
cramping, muscle strains/pulls, upsets your stomach, causes diarrhea,
and/or that we don’t know the long-term side effects of creatine.
There have even been inaccurate reports that creatine was linked to
deaths of some wrestlers and that the FDA was going to ban creatine.
They’re logic has been that since creatine works, there have to be
some side effects. Further, that we shouldn’t be recommending that
athletes take this stuff. After all, many athletes used to take steroids
and then we found out how dangerous they could be. Right?
I have been somewhat amazed at all of the hyperbole and
misinformation regarding creatine supplementation that has appeared in
the popular media over the last number of months. Interestingly, the
scientific community is rather unified in its position about creatine
supplementation (i.e., it works under certain exercise conditions and
that more studies are needed to understand how it works and to continue
to evaluate the medical uses/safety of creatine supplementation). Most
of the negative comments I have seen about creatine have appeared in
newspaper/magazine articles and/or on television. Often, they emanate
from so called "experts" who are apparently not highly
knowledgeable about the creatine literature, have never conducted any
research on creatine (or in some cases no research at all), and/or have
an apparent agenda against nutritional supplementation in general.
It is my view that we must be honest with athletes. Although most
supplements sold to athletes have little to no research supporting their
value, there are some supplements which studies show are effective under
certain conditions (e.g., carbohydrate, creatine, sodium bicarbonate,
sodium phosphate, protein/amino acids, glycerol etc.). In the case of
creatine, it has been one of the most extensively studied nutritional
supplements sold to athletes. There is little doubt that it works under
certain conditions and all available evidence indicates that creatine
supplementation is safe when taken at the recommended dosages.
Nevertheless, a number of coaches, trainers, dietitians, and
physiologists warn against its use. I am even aware of universities and
high schools "banning" its administration and/or discussion in
weight rooms. While I understand that its easier to tell athletes that
supplements don’t work, that they may potentially be dangerous, and/or
that supplements are a waste of money, in the case of creatine, this
view is inconsistent with the available scientific literature. It is my
view that comments about creatine should be based on the scientific
literature, not speculation, untested hypotheses, or unsubstantiated
fear. Those considering using creatine supplements should understand
what it does and doesn’t do so that they can weigh the potential
benefits against risks (if any). The following discusses the clinical
effects of creatine on the body and the validity of anecdotally reported
side effects.
Clinical Effects of Creatine
Supplementation
When someone takes a 5 g dose of creatine, serum creatine levels
typically increase for several hours.7,47,72 This is why
during the loading phase creatine should be ingested every 4 to 6 hours
(4 to 5 times per day). Creatine storage into the muscle primarily
occurs during the first several days of creatine supplementation.47,91
Thereafter, excess creatine that is ingested is primarily excreted as
creatine in the urine with small amounts converted to creatinine and
urea.7,17,47,91 Serum creatinine levels have been reported to
be either not affected 2,25 or slightly increased 64,95
following 28-d, 64 56-d 2,25 and 365-d 95
of creatine supplementation. The increased serum and urinary creatinine
have been suggested to reflect an increased release and cycling of
intramuscular creatine as a consequence of enhanced muscle protein
turnover in response to creatine supplementation and not of pathologic
origin.7,25,47,59 Yet, these increases have been a source of
concern by some physicians in case reports of an athlete68 or
a patient with renal disease88 taking creatine. The reason
for this is that large elevations in serum and urinary creatinine levels
are basic markers of tissue degradation and/or kidney stress. However,
these reports have been criticized because intense exercise and
dehydration increases serum and urinary creatinine levels.41
Consequently, in people who exercise, these increases reflect a greater
breakdown of muscle protein and are completely normal. It makes sense
then that if creatine supplementation allows an athlete to train harder,
creatinine levels may be slightly elevated as the athlete may experience
greater net protein degradation. Some studies which have administered
creatine to athletes during training have reported slight increases in
serum creatinine (e.g. 1.2 to 1.4 µmol/L).64 Interestingly
though, several studies which involved creatine supplementation without
training have found no effects on serum or urinary creatinine levels.75
These findings provide some indirect evidence that the elevations in
creatinine are related to a greater ability to train harder rather than
of pathological origin.
Along these same lines, several studies have evaluated the effects of
creatine supplementation on muscle and liver enzyme levels. Muscle and
liver enzymes increase in response to exercise training. These enzymes
may also be elevated in response to degenerative muscle and/or liver
disease. Studies show that creatine supplementation either has no effect
2,95 or may moderately increase creatine kinase (CK),
2,64 lactate dehydrogenase (LDH),64 and/or aspartate
amino transferase (AST)64 levels following 28-d and 56-d of
supplementation. The increased CK, LDH and AST levels reported following
creatine supplementation were within normal limits for athletes engaged
in heavy training and may reflect a greater concentration/activity of CK
and/or ability to maintain greater training volume.7,59,60,121
Interestingly, in studies in which creatine was administered in subjects
not undergoing intense training, creatine supplementation does not
appear to affect serum muscle enzyme efflux.2,69,70,75
Creatine supplementation has also been reported to positively
affect lipid profiles in middle-aged male and female hypertriglyceremic
patients 25 and trained male athletes.64 In this
regard, Earnest and colleagues 25 reported that 56-d of
creatine supplementation resulted in significant decreases in total
cholesterol (-5 and -6% at day 28 and 56, respectively) and
triglycerides (-23 and -22% at day 28 and 56, respectively) in mildly
hypertriglyceremic patients. A similar response was observed with very
low density lipoproteins (VLDL). In addition, Kreider and coworkers 64
reported that 28-d of creatine supplementation increased high density
lipoproteins (HDL) by 13%, while decreasing VLDL (-13%) and the ratio of
total cholesterol to HDL (-7%). Although additional research is
necessary, these findings suggest that creatine supplementation may
posses health benefit by improving blood lipid profiles.
An extensive amount of research has been conducted on the potential
medical benefits of intravenous PCr administration and oral creatine
supplementation. In this regard, intravenous PCr administration has been
reported to improve myocardial metabolism and reduced the incidence of
ventricular fibrillation in ischemic heart patients.3,19,20,83,93,118,119
The reason for this is that PCr appears to enhance the viability of the
ischemic cell membrane thereby minimizing injury cell during ischemia.
Consequently, there has been interest in determining the effects of oral
creatine supplementation on heart function and exercise capacity in
patients with heart disease. Gordon and associates 38 reported
that creatine supplementation (20 g/d for 10-d) did not improve ejection
fraction in heart failure patients with an ejection fraction less than
40%. However, creatine supplementation significantly increased one
legged knee extension exercise performance (21%), peak torque (5%) and
cycle ergometry performance (10%).
Creatine supplementation has also been used to treat patients with
mitochondrial cytopathies (a condition which reduces exercise capacity)
and infants with in-born errors in creatine synthesis. For example,
Tarnapolosky et al.107 reported that creatine supplementation
(5 g/d for 14-d followed by 2 g/d for 7-d) significantly increased
anaerobic and high-intensity aerobic exercise capacity in patients with
mitochondrial cytopathy. Moreover, several case reports have been
published in the medical literature which indicate that creatine
supplementation (4 to 8 g/d for up to 25 months) allows infants with
inborn errors in creatine synthesis to develop more mentally and
physically normal.4,34,99-103 Collectively, these findings
suggest that intravenous PCr administration and/or oral creatine
supplementation for up to 25 months in duration is safe and may posses
some therapeutic value to certain patient populations.
What’s the bottom line? If you take creatine your serum and urinary
creatine levels will increase for several hours after supplementation.
Without training, there appears to be little if any impact on serum and
urinary creatinine, muscle and liver enzymes, or blood pressure.75,84
However, if you take creatine during training you may observe an
increase in serum creatinine, CK, LDH and possibly AST. These elevations
appear to be related to excess creatine being excreted and/or due to a
greater ability to train harder following creatine supplementation. You
may also experience some positive effects on your blood lipid profiles.
Although additional research is necessary to evaluate the long-term
effects of creatine supplementation on medical status, available studies
suggest that creatine supplementation for up to 2 years is medically
safe and may provide health benefit for various populations when taken
at dosages described in the literature.
Side Effects
The only side effect reported from clinical studies investigating
dosages of 1.5 to 25 g/d for 3- to 365-days in preoperative and
post-operative patients, untrained subjects, and elite athletes has been
weight gain.7,59,60,121 However, a number of
concerns about possible side effects of creatine supplementation have
been mentioned in lay publications, supplement advertisements, and on
Internet mailing lists. It should be noted that these concerns emanate
from unsubstantiated anecdotal reports and may be unrelated to creatine
supplementation. There is no evidence from any well-controlled
clinical study indicating that creatine supplementation causes any of
these side effects. However, one must also consider that although
researchers are required to report side effects in scientific
publications, few long-term studies on creatine supplementation have
been conducted. Consequently, discussion about possible side
effects is warranted.
Some concern has been raised whether creatine supplementation may
suppress endogenous creatine synthesis. Studies have reported that it
takes about four weeks after cessation of creatine supplementation for
muscle creatine 32 and phosphocreatine 115 levels
to return to normal. While it is unclear whether muscle creatine or
phosphocreatine content falls below normal thereafter, there is no
evidence that creatine supplementation causes a long-term suppression of
creatine synthesis.7,50
Since creatine is an amino acid, it has been suggested that creatine
supplementation may increase renal stress or cause liver damage.
However, no studies have reported clinically significant elevations in
liver enzymes in response to creatine supplementation.2,64
Further, Poortmans and colleagues 86 reported that short-term
creatine supplementation (20 g/d for 5-d) does not affect markers of
renal stress. Moreover, preliminary results reported at the 1998
American College of Sports Medicine annual meeting from this group
indicate that longer term creatine supplementation (9 weeks) does not
affect markers of renal stress. Consequently, there is no evidence that
creatine supplementation increases renal stress when taken at
recommended dosages.
There have also been some anecdotal claims that athletes training
hard in hot or humid conditions may experience a greater incidence of
severe muscle cramps and/or muscle injury when taking creatine. However,
no study has reported that creatine supplementation causes cramping,
dehydration, changes in electrolyte concentrations, or increases
susceptibility to muscle strains/pulls even though some of these studies have evaluated highly trained
athletes undergoing intense training 14,36,45,48,57,61,63-66,73,78,91,104,110,116
in hot/humid environments. 36,61,63,65,104 For example, data
that we recently presented at the 1998 National Strength and
Conditioning Association indicated no reports of muscle cramping or
injury in athletes involved in our previous creatine studies.67
Most creatine researchers feel that these observations are overblown.
Finally, concern has been expressed regarding unknown long-term side
effects. While long-term (> 1 year) well-controlled clinical trials
have yet to be performed, it should be noted that athletes have been
using creatine as a nutritional supplement since the mid 1960s. Yet,
this author is not aware of any significant medical complications that
have been directly linked to creatine supplementation. Additionally,
preliminary data presented at the 1998 American College of Sports
Medicine Annual Meeting from Dr. Mike Stone’s laboratory indicate that
long-term creatine supplementation (up to 2 years) does not result in
any abnormal clinical outcome in comparison to controls. Consequently,
from the literature currently available, creatine supplementation
appears to be medically safe when taken at dosages described in the
literature.
Summary
and Conclusions
Based on available research, short-term creatine supplementation may
improve maximal strength/power by 5 to 15%, work performed during sets
of maximal effort muscle contractions by 5 to 15%, single-effort sprint
performance by 1 to 5%, and work performed during repetitive sprint
performance by 5 to 15%. Moreover, long-term supplementation of creatine
or creatine containing supplements (15 to 25 g/d for 5 to 7-d and 2 to
25 g/d thereafter for 7 to 140-d) may promote significantly greater
gains in strength, sprint performance, and fat free mass during training
in comparison to matched-paired controls. However, not all studies have
reported ergogenic benefit possibly due to differences in subject
response to creatine supplementation, length of supplementation,
exercise criterion evaluated, and/or the amount of recovery observed
during repeated bouts of exercise. The only side effect from creatine
supplementation reported in the scientific literature from
studies lasting up to two years in non-athletes, athletes, and patient
populations has been weight gain. Consequently, creatine supplementation
appears to be a safe and effective nutritional strategy to enhance
exercise performance and promote muscle hypertrophy.
Please send us your feedback
on this article.
Richard B. Kreider, PhD, FACSM
rkreider@memphis.edu
References
1. Almada A, Kreider R, Ferreira M, Wilson M,
Grindstaff P, Plisk S, Reinhardy J, Cantler E. Effects of calcium
ß-HMB supplementation with or without creatine during training on
strength and sprint capacity. FASEB J 1997;11:A374. Abstract
2. Almada A, Mitchell T, Earnest C. Impact of chronic
creatine supplementation on serum enzyme concentrations. FASEB J
1996;10:A4567. Abstract
3. Andrews R, Greenhaff P, Curtis S, Perry A, Cowley
AJ. The effect of creatine supplementation on skeletal muscle metabolism
in congestive heart failure. Eur Heart J. 1998;19:617-622.
4. Arias-Mendoza F, Konchanin LM, Grover WD,
Salganicoff L, Selak MA, Brown TR. Possible creatine synthesis deficit
studied by in vivo magnetic resonance spectroscopy. Med Sci Sports
Exerc. 1998;30:S234. Abstract.
5. Balsom P, Ekblom B, Sjodin B, Hultman E. Creatine
supplementation and dynamic high-intensity intermittent exercise. Scand
J Med Sci Sport 1993;3:143-9.
6. Balsom P, Harridge S, Söderlund K, Sjodin B,
Ekblom B. Creatine supplementation per se does not enhance endurance
exercise performance. Acta Physiol Scand 1993;149:521-3.
7. Balsom P, Söderlund K, Ekblom B. Creatine in
humans with special references to creatine supplementation. Sports Med
1994;18:268-80.
8. Balsom P, Söderlund K, Sjödin B, Ekblom B.
Skeletal muscle metabolism during short duration high-intensity
exercise: influence of creatine supplementation. Acta Physiol Scand
1995;1154:303-10.
9. Barnett C, Hinds M, Jenkins D. Effects of oral
creatine supplementation on multiple sprint cycle performance. Aust J
Sci Med. Sport 1996;28:35-9.
10. Becque B, Lochmann J, Melrose D. Effect of
creatine supplementation during strength training on 1 RM and body
composition. Med Sci Sport Exerc 1997;29:S146. Abstract
11. Bessman S, Savabi F. The role of the
phosphocreatine energy shuttle in exercise and muscle hypertrophy. In:
Taylor A, Gollnick P, Green H editors. International Series on Sport
Sciences: Biochemistry of Exercise VII: Champaign, IL: Human Kinetics,
1988:167-78.
12. Birch R, Noble D, Greenhaff P. The influence of
dietary creatine supplementation on performance during repeated bouts of
maximal isokinetic cycling in man. Eur J Appl Physiol 1994;69:268-70.
13. Bosco C, Tihanyi J, Pucspk J, Kovacs I, Gobossy A,
Colli R, Pulvirenti G, Tranquilli C, Foti C, Viru M, Viru A. Effect of
oral creatine supplementation on jumping and running performance. Int J
Sports Med 1997;18:369-72.
14. Burke L, Pyne D, Telford R. Effect of Oral
creatine supplementation on single-effort sprint performance in elite
swimmers. Int J Sport Nutr. 1996;6:222-33.
15. Brannon,T. Effects of creatine loading and
training on running performance and biochemical properties of rat
muscle. Med Sci Sport Exerc 1997;29:489-95.
16. Casey A, Constantin-Teodosiu D, Howell D, Hultman
E, Greenhaff P. Creatine ingestion favorably affects performance and
muscle metabolism during maximal exercise in humans. Am J Physiol
1996;271:E31-7. Abstract
17. Chanutin A. The fate of creatine when administered
to man. J Biol Chem 1926;67:29-41.
18. Chetlin R, Schoenleber J, Bryner R, Gordon P,
Ullrich I, Yeater R. The effects of two forms of oral creatine
supplementation on anaerobic performance during the Wingate test. J Str
Cond Res. 1998;12:In press. Abstract
19. Constantin-Teodosiu D, Greenhaff P, Gardiner S,
Randall M, March J, Bennett T. Attenuation by creatine of myocardial
metabolic stress in Brattleboro rats caused by chronic inhibition of
nitric oxide synthase. Br J Pharmacol 1995;116:3288-92.
20. Conway M, Clark J editors. Creatine and Creatine
Phosphate: Scientific and Clinical Perspectives. San Diego, CA: Academic
Press, 1996.
21. Cooke W., Barnes W. The influence of recovery
duration on high-intensity exercise performance after oral creatine
supplementation. Can J Appl Physiol 1997;22:454-67.
22. Cooke W, Grandjean P, Barnes W. Effect of oral
creatine supplementation on power output and fatigue during bicycle
ergometry. J Appl Physiol 1995;78:670-3.
23. Cordain L. Does creatine supplementation enhance
athletic performance? J Am Coll Nutr 1998;17:205-206.
24. Dawson B, Cutler M, Moody A, Lawrence S, Goodman
C, Randall N. Effects of oral creatine loading on single and repeated
maximal short sprints. Aust J Sci Med Sport 1995;27:56-61.
25. Earnest C, Almada A, Mitchell T. High-performance
capillary electrophoresis-pure creatine monohydrate reduces blood lipids
in men and women. Clin Sci 1996;91:113-18.
26. Earnest C, Almada A, Mitchell T. Effects of
creatine monohydrate ingestion on intermediate duration anaerobic
treadmill running to exhaustion. J Str Cond Res 1997;11:234-8.
27. Earnest C, Beckham S, Whyte BO, Almada AL. Effect
of acute creatine ingestion on anaerobic performance. Med Sci Sports
Exerc. 1998;30:S141. Abstract.
28. Earnest C, Beckham S, Whyte BO, Almada AL. Acute
creatine monohydrate ingestion and anaerobic performance in men and
women. J Str Cond Res. 1998; 12:In press. Abstract
29. Earnest C, Snell P, Rodriguez R, Almada A,
Mitchell T. The effect of creatine monohydrate ingestion on anaerobic
power indices, muscular strength and body composition. Acta Physiol
Scand 1995;153:207-9.
30. Earnest C, Stephens D, Smith J. Creatine ingestion
effects time to exhaustion during estimation of the work rate-time
relationship. Med Sci Sport Exerc 1997;29:S285. Abstract
31. Englehardt, M., Neumann G., Berbalk, A., Reuter,
I. Creatine supplementation in endurance sports. Med Sci Sports Exerc
1998;30:1123-1129.
32. Febbraio M, Flanagan T, Snow R, Zhao S, Carey M.
Effect of creatine supplementation on intramuscular TCr, metabolism and
performance during intermittent, supramaximal exercise in humans. Acta
Physiol Scand 1995;155:387-95.
33. Ferreira M, Kreider R, Wilson M, Grindstaff P,
Plisk S, Reinhardy J, Cantler E, Almada A. Effects of ingesting a
supplement designed to enhance creatine uptake on strength and sprint
capacity. Med Sci Sport Exerc 1997;29:S146. Abstract
34. Ganesan V, Johnson A, Connelly A, Eckhardt S,
Surtees RA. Guanidinoacetate methyltransferase deficiency: new clinical
features. Pediatr Neurol 1997;17:155-157.
35. Gilliam JD, Hohzom C, Martin AD. Effect of oral
creatine supplementation on isokinetic force production. Med Sci Sports
Exerc. 1998;30:S140. Abstract.
36. Godly A, Yates J. Effects of creatine
supplementation on endurance cycling combined with short, high-intensity
bouts. Med Sci Sport Exerc 1997;29:S251. Abstract
37. Goldberg P, Bechtel P. Effects of low dose
creatine supplementation on strength, speed and power by male athletes.
Med Sci Sport Exerc 1997;29:S251. Abstract
38. Gordon A, Hultman E, Kaijser L, Kristgansson S,
Rolf C, Nyquist O, Sylven C. Creatine supplementation in chronic heart
failure increases skeletal muscle creatine phosphate and muscle
performance. Cardiovasc Res 1995;30:413-18.
39. Green A, Sewell D, Simpson L, Hulman E, Macdonald
I, Greenhaff P. Creatine ingestion augments muscle creatine uptake and
glycogen synthesis during carbohydrate feeding in man. J Physiol
1996;491:63. Abstract
40. Green A, Simpson E, Littlewood J, Macdonald I,
Greenhaff P. Carbohydrate ingestion augments creatine retention during
creatine feedings in humans. Acta Physiol Scand 1996;158:195-202.
41. Greenhaff P. Renal dysfunction accompanying oral
creatine supplements. Lancet. 1998; 352:233-234.
42. Greenhaff P, Bodin K, Harris R, Hultman E, Jones
D, McIntyre D, Soderlund K, Turner, DL. The influence of oral creatine
supplementation on muscle phosphocreatine resynthesis following intense
contraction in man. J Physiol 1993;467:75P. Abstract
43. Greenhaff P, Bodin K, Söderlund K, Hultman E.
Effect of oral creatine supplementation on skeletal muscle
phosphocreatine resynthesis. Am J Physiol. 1994;266:E725-30.
44. Greenhaff P, Casey A, Short A, Harris R,
Söderlund K, Hultman E. Influence of oral creatine supplementation of
muscle torque during repeated bouts of maximal voluntary exercise in
man. Clin Sci 1993;84:565-71.
45. Grindstaff P, Kreider R, Bishop R, Wilson M, Wood
L, Alexander C, Almada A. Effects of creatine supplementation on
repetitive sprint performance and body composition in competitive
swimmers. Int J Sport Nutr 1997;7:330-46.
46. Hamilton-Ward K, Meyers M, Skelly W, Marley R,
Saunders J. Effect of creatine supplementation on upper extremity
anaerobic response in females. Med Sci Sport Exerc 1997;29:S146.
Abstract
47. Harris R, Söderlund K, Hultman E. Elevation of
creatine in resting and exercised muscle of normal subjects by creatine
supplementation. Clin Sci 1992;83:367-74.
48. Harris R, Viru M, Greenhaff P, Hultman E. The
effect of oral creatine supplementation on running performance during
maximal short term exercise in man. J Physiol 1993;467:74P. Abstract
49. Hultman E, Bergstrom J, Spriet L, Söderlund K.
Energy metabolism and fatigue. In: Taylor A, Gollnick P, Green H,
editors. Biochemistry of Exercise VII. Champaign, IL: Human Kinetics,
1990:73-92.
50. Hultman E, Söderlund K, Timmons J, Cederblad G,
Greenhaff P. Muscle creatine loading in man. J Appl Physiol
1996;81:232-7.
51. Ingwall J. Creatine and the control of
muscle-specific protein synthesis in cardiac and skeletal muscle. Circ
Res 1976;38:I115-23.
52. Jacobs I, Bleue S, Goodman J. Creatine ingestion
increases anaerobic capacity and maximum accumulated oxygen deficit. Can
J Appl Physiol 1997;22:231-43.
53. Javeirre C, Lizarraga MA, Ventura JL, Garrido E,
Segura R. Creatine supplementation does not improve physical performance
in a 150 m race. Rev Esp Fisiol. 1997;53:343-348.
54. Johnson K, Smodic B, Hill R. The effects of
creatine monohydrate supplementation on muscular power and work. Med Sci
Sport Exerc 1997;29:S251. Abstract
55. Jones AM, Atter T, George KP. Oral creatine
supplementation improves multiple sprint performance in elite ice-hockey
players. Med Sci Sports Exerc. 1998;30:S140. Abstract.
56. Knehans A, Bemben M, Bemben D, Loftiss D. Creatine
supplementation affects body composition and neuromuscular performance
in football athletes. FASEB J. 1998;A863. Abstract
57. Kirksey K, Warren B, Stone M, Stone M, Johnson R.
The effects of six weeks of creatine monohydrate supplementation in male
and female track athletes. Med Sci Sport Exerc 1997;29:S145. Abstract
58. Kreider R. Effects of creatine loading on muscular
strength and body composition. Str Cond 17:72-3, 1995.
59. Kreider, R.B. Creatine, the next ergogenic
supplement? In Sportscience Training & Technology, Internet Society
for Sport Science. Available:
http://www.sportsci.org/traintech/creatine/rbk.html 1998.
60. Kreider, R. B. Creatine supplementation: Analysis
of ergogenic value, medical safety, and concerns. Journal of Exercise
PhysiologyOnline. 1(1): 7-19, 1998. Available:
http://www.css.edu/users/tboone2/asep/jan3.htm
61. Kreider R, Ferreira M, Wilson M, Almada A. Effects
of creatine supplementation with and without glucose on body composition
in trained and untrained men and women. J. Str Cond Res. 1997;11:283.
Abstract
62. Kreider R, Ferreira M, Wilson M, Grindstaff P,
Plisk S, Reinhardy J, Cantler E, Almada A. Effects of ingesting a
supplement designed to enhance creatine uptake on body composition
during training. Med Sci Sport Exerc 1997;29:S145. Abstract
63. Kreider R, Ferreira M, Wilson M, Grindstaff P,
Plisk S, Reinhardy J, Cantler E, Almada A. Effects of calcium ß-HMB
supplementation with or without creatine during training on strength and
sprint capacity. FASEB J 1997;11:A374. Abstract
64. Kreider R, Ferreira M, Wilson M, Grindstaff P,
Plisk S, Reinhardy J, Cantler E, Almada A. Effects of creatine
supplementation on body composition, strength and sprint performance.
Med Sci Sport Exerc 1998;30:73-82.
65. Kreider R, Grindstaff P, Wood L, Bullen D, Klesges
R, Lotz D, Davis M, Cantler E, Almada A.. Effects of ingesting a
lean mass promoting supplement during resistance training on isokinetic
performance. Med Sci Sport Exerc 1996;28:S36. Abstract
66. Kreider R, Klesges R, Harmon K, Grindstaff P,
Ramsey L, Bullen D, Wood L, Li Y, Almada A. Effects of ingesting
supplements designed to promote lean tissue accretion on body
composition during resistance exercise. Int J Sport Nutr 1996;6:234-46.
67. Kreider R, Rasmussen C, Ransom J, Almada A.
Effects of creatine supplementation during training on the incidence of
muscle cramping, injuries, and GI distress. J Str Cond Res. 1998; 12:In
press. Abstract
68. Kuehl K, Goldberg L, Elliot D. Renal insufficiency
after creatine supplementation in a college football athlete. Med Sci
Sports Exerc. 1998;30:S235. Abstract.
69. Kurosawa Y, Iwane H, Hamaoka T, Shimomitsu T,
Katsumura T, Sako T, Kuwamon M, Kimura N. Effects of oral creatine
supplementation on high-and low-intensity grip exercise performance. Med
Sci Sport Exerc 1997;29:S251. Abstract
70. Kurosawa Y, Katsumura T, Hamoaka T, Sako T,
Kuwamori M, Kimura N, Shimomitsu T. Effects of oral creatine
supplementation on localized muscle performance and muscle creatine
phosphate concentration. Jap J Phys Fit Sports Med. 1998;47:361-366.
71. Lefavi RG, McMillan JL, Kahn PJ, Crosby JF,
Digioacchino RF, Streater JA. Effects of creatine monohydrate on
performance of collegiate baseball and basketball players. J Str Cond
Res. 1998; 12:In press. Abstract
72. Lemon P, Boska M, Bredle D, Rogers M, Ziegenfuss
T, Newcomer B. Effect of oral creatine supplementation on energetic
during repeated maximal muscle contraction. Med Sci Sport Exerc
1995;27:S204. Abstract
73. Leenders N, Lesniewski L, Sherman W, Sand G, Sand
S, Mulroy M, Lamb D. Dietary creatine supplementation and swimming
performance. Overtraining and Overreaching in Sport Conference
Abstracts. 1996;1:80. Abstract
74. Michaelis J, Vukovich M. Effect of two different
forms of creatine supplementation on muscular strength and power. Med
Sci Sports Exerc. 1998;30:S272. Abstract.
75. Mihic S, MacDonald JR, McKenzie S, Tarnopolsky MA.
The effect of creatine supplementation on blood pressure, plasma
creatine kinase, and body composition. FASEB J. 1998;12:A652. Abstract
76. Miszko TA, Baer JT, Vanderburgh PM. The effect of
creatine loading on body mass and vertical jump of female athletes. Med
Sci Sports Exerc. 1998;30:S141. Abstract.
77. Mujika I, Padilla S. Creatine supplementation as
an ergogenic aid for sports performance in highly trained athletes: a
critical review. Int J Sports Med. 1997;18:491-496.
78. Mujika I, Chatard J, Lacoste L, Barale F, Geyssant
A. Creatine supplementation does not improve sprint performance in
competitive swimmers. Med Sci Sport Exerc 1996;28:1435-41.
79. Myburgh K, Bold A, Bellinger B, Wilson G, Noakes
T. Creatine supplementation and sprint training in cyclists: metabolic
and performance effects. Med. Sci. Sport Exerc. 1996;28:S81. Abstract
80. Nelson A, Day R, Glickman-Weiss E, Hegstad M,
Sampson B. Creatine supplementation raises anaerobic threshold. FASEB J
1997;11:A589. Abstract
81. Odland L, MacDougall J, Tarnopolsky M, Elorriage
A, Borgmann A. Effect of oral creatine supplementation on muscle [PCr]
and short-term maximum power output. Med Sci Sport Exerc
1997;29:216-219.
82. Oopik V, Paasuke M, Timpamann S, Medijainen L,
Ereline J, Smirnova T. Effect of creatine supplementation during rapid
body mass reduction on metabolism and isokinetic muscle performance
capacity. Eur J Appl Physiol 1998;78:83-92.
83. Pauletto P, Strumia E. Clinical experience with
creatine phosphate therapy. In Conway M and Clark J. editors. Creatine
and Creatine Phosphate: Scientific and Clinical Perspectives. San Diego,
CA: Academic Press, 1996:185-98.
84. Peeters BM, Lantz CD, Mayhew JL. Effect of oral
creatine monohydrate and creatine phosphate supplementation on maximal
strength indices, body composition, and blood pressure. J Str Cond Res.
1998; 12:In press.
85. Peyrebrune MC, Nevill ME, Donaldson FJ, Cosford
DJ. The effects of oral creatine supplementation on performance in a
single and repeated sprint swimming. J Sports Sci. 1998; 16:271-279.
86. Poortmans J, Auquier H, Renaut V, Durassel A,
Saugy M, Brisson G. Effect of short-term creatine supplementation on
renal responses in men. Eur J Appl Physiol 1997;76:566-7.
87. Prevost M, Nelson A, Morris G. The effects of
creatine supplementation on total work output and metabolism during
high-intensity intermittent exercise. Res Q Exerc Sport 1997;68:233-40.
88. Pritchard NR, Kaira PA. Renal dysfunction
accompanying oral creatine supplements. Lancet 1998 Apr
25;351(9111):1252-1253.
89. Rawson ES, Clarkson PM, Melanson EL. The effects
of oral creatine supplementation on body mass, isometric strength, and
isokinetic performance in older individuals. Med Sci Sports Exerc.
1998;30:S140. Abstract.
90. Redondo D, Dowling E, Graham B, Almada A, Williams
M. The effect of oral creatine monohydrate supplementation on running
velocity. Int J Sport Nutr 1996;6:213-21.
91. Rossiter H, Cannell E, Jakeman P. The effect of
oral creatine supplementation on the 1000-m performance of competitive
rowers. J Sports Sci 1996;14:175-9.
92. Ruden T, Parcell A, Ray M, Moss K, Semler J, Sharp
R, Rolfs G, King D. Effects of oral creatine supplementation on
performance and muscle metabolism during maximal exercise. Med Sci Sport
Exerc 1996;28:S81. Abstract
93. Saks V, Stepanov V, Jaliashvili I, Konerev E,
Kryzkanovsky S, Strumia E. Molecular and cellular mechanisms of action
for cardioprotective and therapeutic role of creatine phosphate. In
Conway M, Clark J editors. Creatine and Creatine Phosphate: Scientific
and Clinical Perspectives. San Diego, CA: Academic Press, 1996:91-114.
94. Schneider D., McDonough P, Fadel P, Berwick J.
Creatine supplementation and the total work performed during 15-s and
1-min bouts of maximal cycling. Aust J Sci Med Sport. 1997;29(3):65-8.
95. Sipila I, Rapola J, Simell O, Vannas A.
Supplementary creatine as a treatment for gyrate atrophy of the choroid
and retina. New Eng J Med 1981;304:867-70.
96. Smart NA, McKenzie SG, Nix LM, Baldwin SE, Page K,
Wade D, Hampson PK. Creatine supplementation does not improve repeat
sprint performance in soccer players. Med Sci Sports Exerc.
1998;30:S140. Abstract.
97. Smith JC, Stephens DP, Hall EL, Jackson AW,
Earnest CP. Effect of oral creatine ingestion on parameters of the work
rate-time relationship and time to exhaustion in high-intensity cycling.
Eur J Appl Physiol. 1998;77:360-365.
98. Stevenson SW, Dudley GA. Creatine supplementation
and resistance exercise. J Str Cond Res. 1998; 12:In press. Abstract
99. Stockler S, Hanefeld F. Guanidinoacetate
methyltransferase deficiency: a newly recognized inborn error of
creatine biosynthesis. Wien Klin Wochenschr 1997 Feb 14;109(3):86-88.
100. Stockler S, Hanefeld F, Frahm J. Creatine
replacement therapy in guanidinoacetate methyltransferase deficiency, a
novel inborn error of metabolism. Lancet. 1996; 21;348:789-790.
101. Stockler S, Holzbach U, Hanefeld F, Marquardt I,
Helms G, Requart M, Hanicke W, Frahm J. Creatine deficiency in the
brain: a new, treatable inborn error of metabolism. Pediatr Res. 1994;
36:409-413.
102. Stockler S, Isbrandt D, Hanefeld F, Schmidt B,
von Figura K. Guanidinoacetate methyltransferase deficiency: the first
inborn error of creatine metabolism in man. Am J Hum Genet.
1996;58:914-922.
103. Stockler S, Marescau B, De Deyn PP, Trijbels JM,
Hanefeld F. Guanidino compounds in guanidinoacetate methyltransferase
deficiency, a new inborn error of creatine synthesis. Metabolism.
1997;46:1189-1193.
104. Stout J, Eckerson J, Noonan D, Moore G, Cullen D.
The effects of a supplement designed to augment creatine uptake on
exercise performance and fat-free mass in football players. Med Sci
Sport Exerc 1997;29:S251. Abstract
105. Stroud M, Holliman D, Bell D, Green A, MacDonald
I, Greenhaff P. Effect of oral creatine supplementation on respiratory
gas exchange and blood lactate accumulation during steady-state
incremental treadmill exercise and recovery in man. Clin Sci
1994;87:707-10.
106. Syrotuik DG, Bell GJ, Burnham R, Sim LL, Calvert
RA, MacLean IM. Absolute ane relative strength performance following
creatine monohydrate supplementation combined with periodized resistance
training. J Str Cond Res. 1998; 12:In press. Abstract
107. Tarnapolosky M, Roy B, MacDonald J. A randomized
controlled trial of creatine monohydrate in patients with mitochondrial
cytopathies. Muscle Nerve 1997;20:1502-9.
108. Terrilion K, Kolkhorst F, Dolgener F, Joslyn S.
The effect of creatine supplementation on two 700-m maximal running
bouts. Int J Sport Nutr 1997;7:138-43.
109. Theoduru A, Cooke CB, King RFGJ, Ducket R. The
effect of combined carbohydrate and creatine ingestion on anaerobic
performance. Med Sci Sports Exerc. 1998;30:S272. Abstract.
110 Thompson C, Kemp G, Sanderson A, Dixon R, Styles
P, Taylor D, Radda G. Effect of creatine on aerobic and anaerobic
metabolism in skeletal muscle in swimmers. Br J Sports Med
1996;30:222-5.
111. Thorensen E, McMillan J, Guion K, Joyner B. The
effect of creatine supplementation on repeated sprint performance. J Str
Cond Res. 1998; 12:In press. Abstract
112. Tullson P, Rundell K, Sabina R, Terjung R.
Creatine analogue beta-guanidinopropionic acid alters skeletal muscle
AMP deaminase activity. Am J Physiol 1996;270:C76-85.
113. Vanakoski J, Kosunen V, Meririnne E, Seppala T.
Creatine and caffeine in anaerobic and aerobic exercise: effects on
physical performance and pharmacokinetic considerations. Int J Clin
Pharmacol Ther. 1998;36:258-262.
114. Vandenberghe K, Gillis N, Van Leemputte M, Van
Hecke P, Vanstapel F, Hespel P. Caffeine counteracts the ergogenic
action of muscle creatine loading. J Appl Physiol 1996;80:452-7.
115. Vanderberghe, K., Goris M., Van Hecke P., Van
Leeputte M., Vangerven L., Hespel P. Long-term creatine intake is
beneficial to muscle performance during resistance-training. J Appl
Physiol 1997;83:2055-63.
116. Volek J, Kraemer W, Bush J, Boetes M, Incledon T,
Clark K, Lynch J. Creatine supplementation enhances muscular performance
during high-intensity resistance exercise. J Am Diet Assoc
1997;97:765-70.
117. Wakatsuki T, Ohira Y, Nakamura K, Asakura T, Ohno
H, Yamamoto M. Changes of contractile properties of extensor digitorum
longus in response to creatine-analogue administration and/or hindlimb
suspension in rats. Jpn J Physiol 1995;45:979-89.
118. Wakatsuki T, Ohira Y, Yasui W, Nakamura K,
Asakura T, Ohno H, Yamamoto M. Responses of contractile properties in
rat soleus to high-energy phosphates and/or unloading. Jpn J Physiol
1994;44:193-204.
119. Walters PH, Olrich TW. The effects of creatine
supplementation on strength performance. J Str Cond Res. 1998; 12:In
press. Abstract
120. Warber JP, Patton JF, Tharion WJ, Montain SJ,
Mello RP, Lieberman HR. Effects of creatine monohydrate supplementation
on physical performance. FASEB J. 1998;12:A1040. Abstract
121. Williams MH, Branch JD. Creatine supplementation
and exercise performance: an update. J Am Coll Nutr. 1998;17:216-234.
122. Wood KK, Zabik RM, Dawson ML, Frye PA. The
effects of creatine monohydrate supplementation on strength, lean body
mass, and circumferences in male weightlifters. Med Sci Sports Exerc.
1998;30:S272. Abstract.
123. Ziegenfuss T, Lemon P, Rogers M, Ross R,
Yarasheski K. Acute creatine ingestion: effects on muscle volume,
anaerobic power, fluid volumes, and protein turnover. Med Sci Sports
Exerc 1997;29:S127. Abstract
124. Ziegunfuss T, Lemon PWR, Rogers M, Ross R,
Yarasheski K. Acute Fluid Volume Changes in Men During Three Days of
Creatine Supplementation. Journal of Exercise Physiology Online.
1998;1:In press.
|
|
|

{kind=link}